nationalbreastcancer.org
|
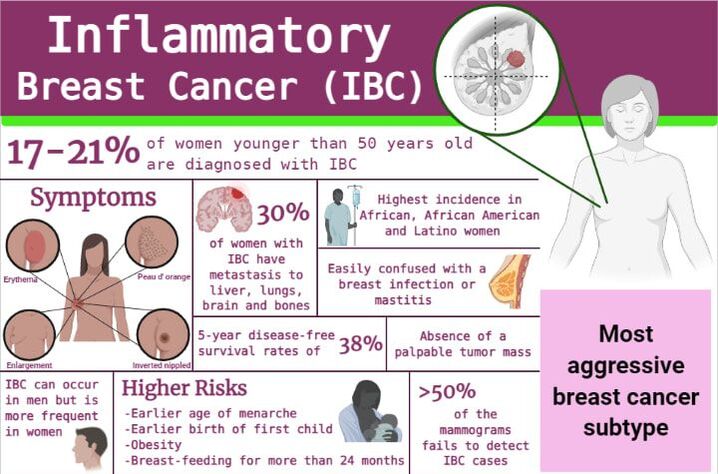
Breast cancer is the second leading cause of death in females in the United States, Inflammatory Breast Cancer (IBC) being the most aggressive subtype. To this date there is no effective targeted therapeutic, especially for those patients that account for approximately 20–40% of IBC cases with a triple‐negative breast cancer (TNBC) classification. Several studies established that molecular signature of IBC shows important differences from the other breast cancer subtypes, such as overexpression of ErbB receptors (EGFR). However, the molecular alterations do not explain completely the aggressive and rapid IBC phenotype.
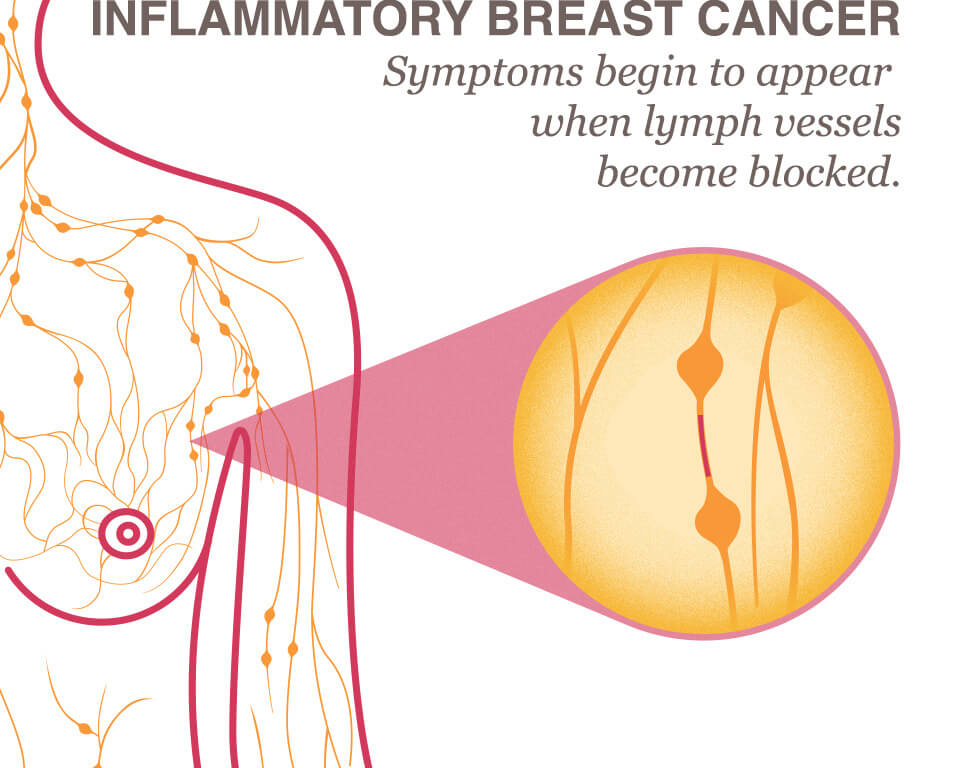
Recently, several studies have shown that estrogen can exert non-genomic effects in triple-negative IBC and other TNBCs, mediated by the expression of alternate estrogen receptors, including ERα36 and GPR30. In this context, estrogen can activate non‐genomic signaling pathways involved in the acquisition of pro-oncogenic phenotypes such as proliferation, invasion and migration in IBC cells. |
|
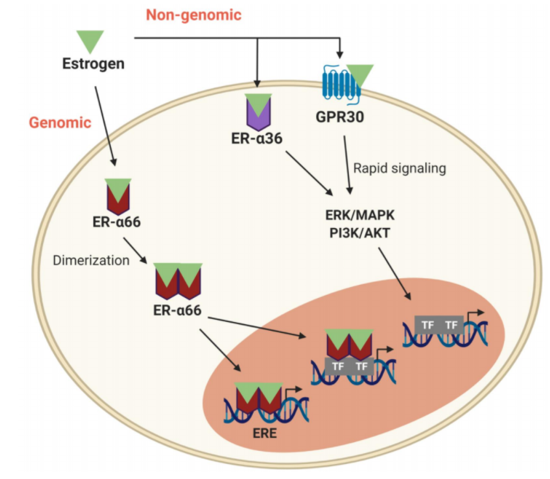
Estrogen non-genomic signaling refers to the rapid action of these alternate estrogen receptors that upon estrogen binding activate protein-kinase cascades in the cytoplasm. Moreover, estrogen can activate the estrogen receptors involved in both genomic and non-genomic signaling pathways. After the dimerization, upon estrogen binding of estrogen receptors, they can act as a transcription factor or can promote its activation and induce gene expression. In contrast, estrogen non-genomic receptors induce the activation of kinases that trigger a rapid action of alternate estrogen receptors and induce the expression of genes involved in pro-oncogenic phenotypes. Estrogen receptor (ER) can bind directly to DNA-specific sequences or indirectly by binding to other transcription factors. Besides, coactivators can participate in ERα activation by crosstalk with other signaling pathways; leading to ERα phosphorylation.
|
|

Hanahan and Weinberg (2011); BioRender.com |
Hallmarks of CancerOriginal hallmarks
Enabling factors Emerging hallmarks 
|
